
I will be discussing Sugar Coated at 1:00 p.m. ET. The link to the conversation is here.
Last week, a Feedback comment from a reader, Judith Rice-Jones, inspired me to try to understand what’s going on with the new heart disease prevention guidelines (I can’t say I’m succeeding very well).
Looking forward to your response to the recent recommendations for more people to take statins. Don’t see anything in the new recommendations about changing lifestyle or diet to reduce risks of stroke or heart attack.
Yes, there are lifestyle recommendations. But lifestyle changes do not make money for drug companies, and they don’t get press attention.
The American College of Cardiology (ACC) and American Heart Association (AHA) issued four sets of guidelines:
These organizations say:
AHA and ACC are pleased to announce a series of new cardiovascular prevention guidelines for the assessment of cardiovascular risk, lifestyle modifications that reduce risk, management of elevated blood cholesterol, and management of increased body weight in adults. These guidelines are based on rigorous, comprehensive, systematic evidence reviews originally sponsored by the NHLBI. The ACC and AHA collaborated with professional organizations to finalize these AHA/ACC cardiovascular prevention guidelines, and stakeholder organizations were invited to review and endorse the final documents.
So these guidelines are a major big deal. The New York Times said you need to know three things about them:
But wait!
As the New York Times also suggested, the new guidelines have taken many by surprise.
This is an understatement.
Problem #1: Authoritative clinicians say more patients should not be taking statins
This announcement is not a result of a sudden epidemic of heart disease, nor is it based on new data showing the benefits of lower cholesterol. Instead, it is a consequence of simply expanding the definition of who should take the drugs — a decision that will benefit the pharmaceutical industry more than anyone else.
This opinion piece points out that members of the group writing the recommendations have financial ties to drug makers, as do both the AHA and ACC.
The guidelines might make sense, they say, if statins
actually offered meaningful protection from our No. 1 killer, heart disease; if they helped people live longer or better; and if they had minimal adverse side effects. However, none of these are the case…as shown in a recent BMJ article co-written by one of us.
Perhaps more dangerous, statins provide false reassurances that may discourage patients from taking the steps that actually reduce cardiovascular disease…80 percent of cardiovascular disease is caused by smoking, lack of exercise, an unhealthy diet, and other lifestyle factors. Statins give the illusion of protection to many people, who would be much better served, for example, by simply walking an extra 10 minutes per day.
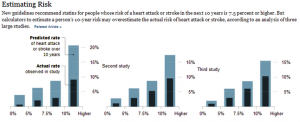
Problem #2: The risk calculator greatly overestimates risk
The lead article in today’s Times summarizes studies to be published in The Lancet tomorrow concluding that the risk calculator makes the risks seem greater than they really are.
![]()
It will lead many doctors to prescribe statin drugs to people who do not need to take them (from the standpoint of drug companies, that’s the point).
The calculator overpredicted risk by 75 to 150 percent, depending on the population. A man whose risk was 4 percent, for example, might show up as having an 8 percent risk. With a 4 percent risk, he would not warrant treatment — the guidelines that say treatment is advised for those with at least a 7.5 percent risk and that treatment can be considered for those whose risk is 5 percent.
What to do?
Just for fun
Let’s let Brian McFadden (Sunday’s New York Times Week in Review) have the last word for today.

I will be discussing Sugar Coated at 1:00 p.m. ET. The link to the conversation is here.
