The federal vision for chronic disease prevention: individual behavior, not the environment
At the insistence of Jerry Mande, I watched the meeting of the President’s Council of Advisors on Science and Technology (PCAST) to learn about the Federal Vision for Advancing Nutrition Science in the United States.
This Vision derives from last year’s White House Conference on Hunger, Nutrition, and Health and its pillar on enhancing nutrition research.
Cathie Woteki, who introduced the report, made a forceful case for the importance of chronic disease prevention. Her committee was shocked that the majority of Americans are overweight or obese, and at a cost of $500 billion annually. She pointed out the lack of focus and coordination of 200 existing programs that ought to be addressing this issue.
The conclusion: not enough research on chronic disease and more funding needed.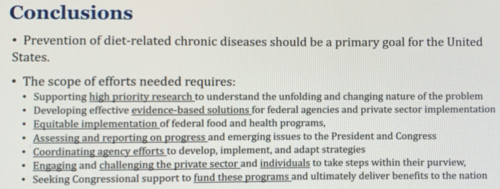
No question about that. Yes, we need more nutrition research and more funding for it. A lot more.
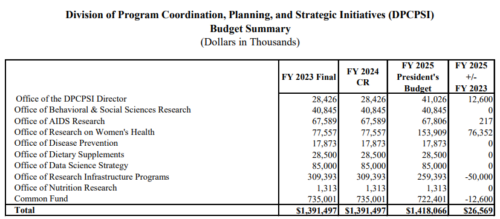
But the White House request for the Office of Nutrition Research is only $1.3 million (see p. 26). Surely this is some kind of joke? It’s hardly even a rounding error in federal terms.
As for the PCAST report’s efforts needed: That’s all?
Yes we can use more data and research on personal eating habits and individual behavior, but what about the food environment?
Maybe PCAST is under political constrainsts but this sure does feel like a lost opportunity.
The report —as yet unpublished—appears to say nothing about:
- The effects of ultra-processed foods on individual food choices and weight. (the word “ultra-processed” was not mentioned)
- The need to change the food environment to make it easier and less expensive for individuals to make healthier food choices.
- Policies to requirie food companies to produce healthier foods and reduce serving sizes.
- Policies to stop the food industry from marketing ultra-processed foods to kids.
- Programs to achieve the existing 2030 health objectives to prevent obesity and chronic disease (these were not mentioned).
The committee said it consulted widely to produce this report. Not widely enough, I’d say.
Compare this to what the UK House of Lords is doing in its hearings on Food, Diet and Obesity. Take a look at who they are listening to.
If the PCAST committee talked to any of these people, their comments are not showing up.
PCAST has a real opportunity here to push for a strong research and policy agenda to address obesity and its related chronic diseases.
What kind? Here are my suggestions.